
A bronchus is a passage of airway in the respiratory tract that conducts air into the lungs. The bronchus branches into smaller tubes called bronchioles. The human trachea divides into two main bronchi (also called mainstem bronchi), that extend laterally (but not symmetrically) into the left and right lung respectively, at the level of the sternum. The point where the trachea divides into the bronchi is called the carina. The right main bronchus is wider, shorter than the left main bronchus, which is thinner and longer. The right main bronchus subdivides into three lobar bronchi, while the left main bronchus divides into two. The lobar bronchi (also called secondary bronchi) divide into tertiary bronchi, each of which supplies air to a different bronchopulmonary segment. Bronchial foreign bodies produce variable pathological conditions and symptoms.
1.Age: Usually children below 3 years of age are most commonly affected
2. In unconscious patients, or patients under anesthesia, accidental aspiration of dentures or loose teeth may occur.
3.Children may accidentally aspirate the foreign body while playing if they have something in their mouth. .
1.Organic foreign bodies: These foreign bodies swell up and gradually increase the airway obstruction and irritation. Example peanuts, peas, apple, chickoo seeds and grains.
2. Inorganic foreign bodies: These includes plastic beads, toys, buttons. These foreign bodies are often longstanding.
1.Early stage: Occurs immediately after the inhalation of the foreign body. There is intense coughing. If the foreign body is large it may cause cyanosis and even death. The foreign body may also be coughed out.
2.Intermediate stage: The patient is relatively symptomless. The period of this stage depends on the size and type of foreign body.
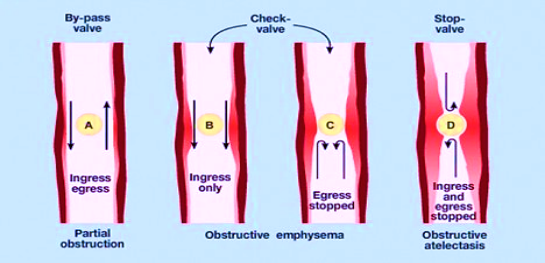
3.Late stage: The symptoms vary from bronchial obstruction, irritation and inflammation.Three types of bronchial obstruction are seen:
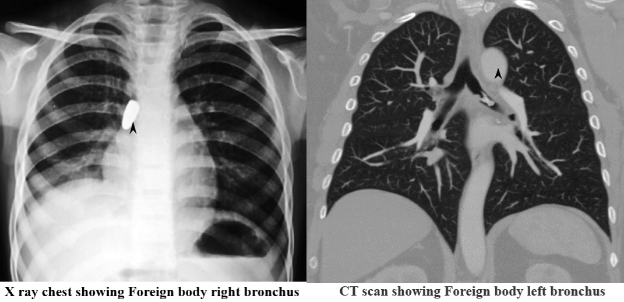
1.HRCT of chest- It is extremely useful in delineating the exact shape, location, volume and form of a bronchial foreign body and can help the surgeon plan for operative bronchoscopy and safe removal of the foreign body. It may reveal the impacted foreign body directly as a hyperdensity in the lumen of airway. It is also possible to differentiate low density foreign bodies from the mucous plug by determining the Hounsfield value. Ancillary findings such as post-obstructive emphysema, collapse, consolidation and bronchiectasis are also well demonstrated.
2. X-ray neck and chest: A radiopaque foreign body may be seen on plain X-ray.
3. X-ray chest may show obstructive emphysema, tracheal shift, collapse and mediastinal shift.
4. CT scan can be done to confirm foreign body bronchus with the exact site of impaction.
1. Bronchoscopy under general anesthesia is performed for all suspected foreign bodies.
2.Fluoroscopic bronchoscopy- This is done when a foreign body has invaded a part of tracheobronchial tree and cannot be safely removed.