
Tinnitus is defined as a sound perceived more than five minutes at a time in the absence of any external acoustic or electrical stimulus to the ear and not occurring immediately after exposure to loud noise, phantom auditory perception, or head noise
There are two types of tinnitus-
1. Subjective tinnitus– Here tinnitus audible only to the patient. May be due to sensorineural hearing loss due to any cause.
2.Objective tinnitus– Here tinnitus audible not only to patient, but also to the examiner. It usually caused by arteriovenous malformations, glomus tumors, palatal or tympanic myoclonus.
I. Vascular somatosounds– Vascular lesions, either arterial or venous, can produce turbulent blood flow, leading to pulsatile somatosounds.
They include:
a) Vascular tumors- Glomus tympanicum or jugular, Hemangioma.
b) Vascular malformations- Arteriovenous malformations, aneurysms, fistulae, carotid artery stenosis, transverse sinus stenosis.
c) Increased intracranial pressure- venous hum.
d) Transmitted cardiac murmurs.
e) Different hyperdynamic vascular states- pregnancy, hyperthyroidism, anaemia.
II. Myogenic somatosounds- The most common forms are palatal and less common middle ear muscles, tensor tympani and stapedial myoclonus.
III. Patulous eustachian tube- It leads to to-and-fro movements of the tympanic membrane, synchronous with nasal respiration which can be perceived as ‘blowing’ sound or their own voice reverberation.
IV. Temporomandibular joint abnormality– It causes audible vibratory sound arising from jaw clenching.
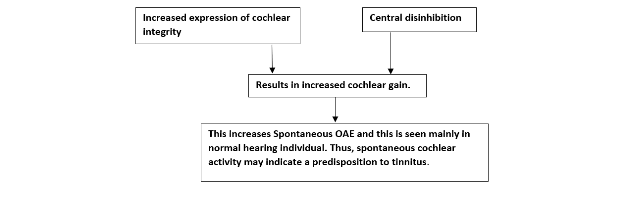
V. Spontaneous otoacoustic emissions can be the reason of tinnitus
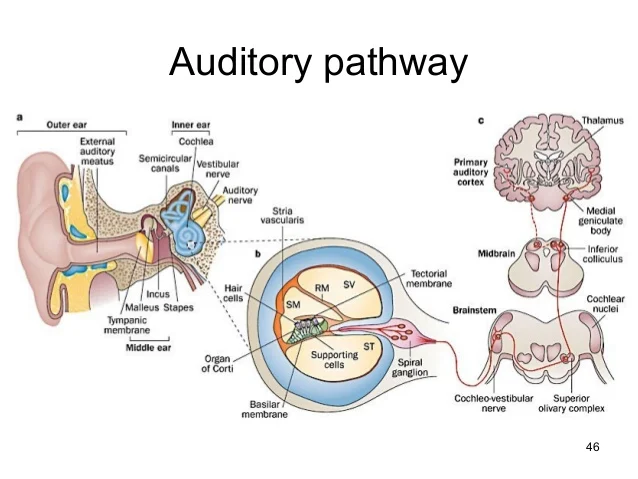
The auditory system consists of two pathways: Afferent pathway-This provides input to the proximal structure of auditory system. This is predominantly excitatory. Efferent pathway-This modulates acoustic information. It is predominantly inhibitory. Any pathological alteration at any one level may have functional consequence at the other levels of the auditory system. Tinnitus is the consequence of the aberrant spontaneous neuronal activity within the auditory system. It can be due to lesion or dysfunction at the level of cochlea to the uppermost level of the auditory system. Tinnitus related neuronal activity triggers feedback mechanism in order to balance between excitation and inhibition and preserve the homeostasis. Tinnitus is characterized by process of habituation, so in most cases the tinnitus gradually attenuates. However, some fail to adopt to habituation leading to persistent tinnitus.
Noise trauma, ototoxicity, ageing results in downregulation of inhibitory activity of GABA on neurotransmitter receptor in central auditory pathway (mostly at cochlear nucleus and inferior colliculus), resulting in increased damage to the auditory system, expressed in form of tinnitus. Mechanism of spontaneous activity and tonotopic
Reorganization:
Treatment with hearing aids and cochlear implant will establish the afferent input, thus reducing tinnitus.