Direct laryngoscopy is a direct visualization of the different parts of the larynx and hypopharynx.
Indications:
Diagnostic:
When indirect laryngoscopy is not possible for example, in young children and infants for laryngeal lesions like stridor.
Vocal cord paralysis.
Extent of the growth in cases carcinoma of the vocal cords and to take a biopsy.
As a part of panendoscopy in cases of unknown primary with cervical metastasis.
Therapeutic:
Excision of benign lesions of the larynx such as papilloma, vocal nodules or cyst.
Insertion of laryngeal stents.
Injection of teflon paste in the vocal cord in cases of vocal cord palsy.
Dilatation of subglottic stenosis.
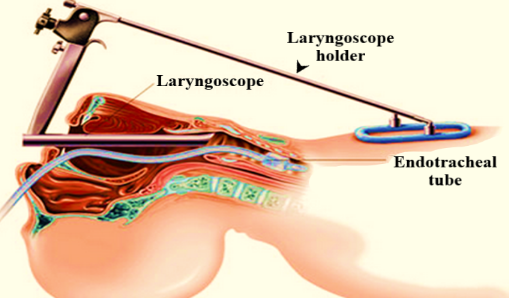
Procedure:
Procedure is done under general anaesthesia. The patient is in Boyce position with flexion of the cervical spine and extension of the atlanto-occipital joint.
The laryngoscope is held in the right hand and inserted into the oval cavity till the epiglottis is visualized. The tip of the epiglottis is lifted with the laryngoscope. The larynx is then visualized.
Structure visualized:
Following structures are examined serially:
Base of tongue.
Median and lateral glossoepiglottic fold.
Right and left valleculae.
Epiglottis (its tip, lingual and laryngeal surfaces).
Right and left pyriform sinuses.
Aryepiglottic folds.
Arytenoids.
Postcricoid region.
Both false cords.
Anterior and posterior commissure.
Right and left ventricles.
Right and left vocal cords.
Subglottic area.
Mobility of vocal cords is also observed.
Complications:
Damage to lips, gums, or tongue.
Damage to the cervical spine.
Anaesthetic complications.
Vasovagal stimulation due to manipulation of the larynx.
However, the above complications are greatly minimised in skilled hands and with good instrumentation setup.