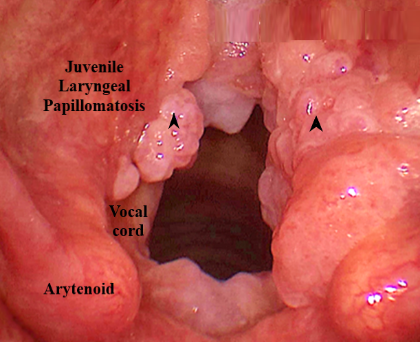
MacKenzie first described this condition 100 years ago. These papillomas affect not only the larynx, but other areas of the respiratory tract, hence they are also called recurrent respiratory papillomatosis.
Immunofluorescent techniques show evidence of human papilloma virus having incorporated into cellular DNA.