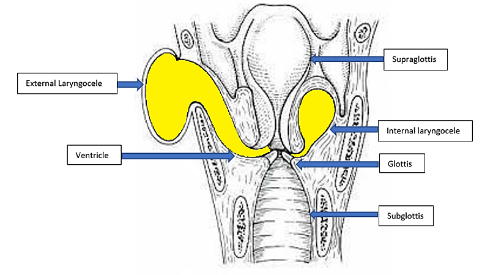
These are air filled cystic swellings due to dilatation of the saccule lined by columnar ciliated epithelium.