It is an excessive flaccidity of the supraglottic portion of the larynx and is the most common cause of congenital stridor.
Aetiology:
Age: The condition manifests at birth or soon after and usually disappears by 2 years of age.
More common in lower socioeconomic patients.
Poor nutrition.
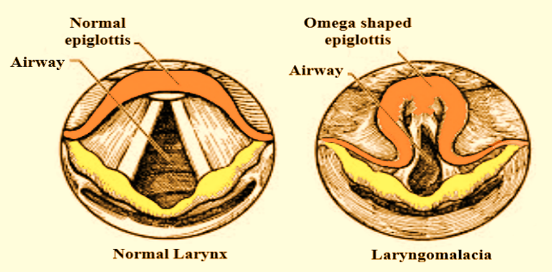
Occurs due to large omega shaped epiglottis, bulky aryepiglottic folds and excessive tissue flaccidity.
Clinical features:
Inspiratory stridor present at birth or even several weeks after birth.
Suprasternal indrawing may be present.
Stridor is worse when the child is supine and better when prone.
Rarely cyanosis and dyspnoea develop.
Stridor often interferes with feeding.
Respiratory infection precipitates the stridor needing urgent treatment.
Treatment:
Treatment of the majority of patients with laryngomalacia is conservative.
In cases of mild or moderate stridor without feeding difficulties, observation is recommended after making a diagnosis. It is important to monitor for weight gain and development of any severe symptoms outlined above.
Positional feeding and thickening feed may help those infants with feeding difficulties.
Conservative management – feeding upright, repeated burping after every feed, anti-reflux therapy with a proton pump inhibitor.
Symptoms abate in the majority of patients by the age of 12 to 18 months without the need for surgical intervention. So, reassurance to parents is necessary.
Antibiotics are given if there is additional bacterial infection of upper respiratory tract.
Vitamin D supplementation.
Nearly 10 to 20% of infants with laryngomalacia will have severe symptoms. These patients often require surgical intervention.
Immediately patient may be relieved by intubation and tracheostomy.
Supraglottoplasty has become the initial treatment of choice for patients with severe symptoms.
Multiple techniques for this procedure exist, including the use of a laser, cold steel, laryngeal microdebrider, or coblator.
The most frequent reasons for surgical intervention are worsening airway symptoms and failure to thrive.
The supraglottoplasty procedure should be individualized to the particular patient’s anatomy but may consist of dividing shortened aryepiglottic folds, removing redundant arytenoid mucosa, performing an epiglottopexy, or a combination of these.
Care should be taken to avoid damage to the interarytenoid mucosa as glottic stenosis can result from scarring of this area.
Steroid administration during surgery and in the postoperative period to decrease airway inflammation is typically the recommended pharmaceutical therapy.