Stridor is the noisy respiration due to obstruction of the air in and out of the lower respiratory tract. It is usually a symptom suggestive of a disease not a disease by itself.
Types of Stridor:
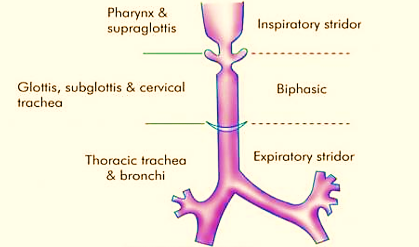
Inspiratory stridor: Seen in obstructive lesions of supraglottis or pharynx, like laryngomalacia or retropharyngeal abscess.
Expiratory stridor: Seen in obstructive lesions of thoracic trachea, primary and secondary bronchi, e.g. bronchial foreign body and tracheal stenosis.
Biphasic stridor: Both inspiratory and expiratory components are seen in the stridor. It is seen lesions of glottis, subglottis and cervical trachea, e.g. laryngeal papillomas, vocal cord paralysis and subglottis stenosis.
Causes of stridor:
a) Congenital:
Laryngeal web.
Laryngomalacia.
Laryngeal stenosis.
Cysts of vocal cords.
b) Inflammatory:
Acute epiglottitis.
Laryngitis.
Laryngeal oedema.
Laryngotracheal bronchitis.
Tetanus.
Ludwig’s angina.
c) Neoplastic:
Juvenile laryngeal papillomatosis.
Carcinoma larynx.
d) Neurological:
Vocal cord palsy.
Tetany (laryngismus stridulus).
e) Trauma:
Burns.
Birth injury.
Intubation trauma.
Diagnosis:
a) Detailed history:
The onset of stridor.
Infective or congenital aetiology.
History of foreign body aspiration.
Hoarseness of voice in the past.
b) Clinical examination:
Upper airway examination for any visible obstructive lesion.
Examination of cardiovascular system.
To note signs of respiratory distress and cyanosis.
Examination of neck for local trauma and injury.
Suprasternal inspiratory in-drawing.
Investigations:
X-ray neck lateral view to see the airway.
X-ray chest.
CT Scan neck and chest to know the exact cause and site of obstruction.
Direct laryngoscopy and fibre optic bronchoscopy to confirm diagnosis.
Angiography may be needed for above vascular anomalies before operation.
Oesophagogram with contrast may be needed for tracheobronchial fistula or aberrant vessels or oesophageal atresia.
Important: Tracheostomy would be useful only in the obstruction above the level of the tracheostomy site not below it.