
Ludwig’s angina is characterized by cellulitis of the floor of the mouth and the submandibular space secondary to soft tissue infection.
Submandibular space lies between mucous membrane of the floor of mouth and tongue on one side and superficial layer of deep cervical fascia extending between the hyoid bone and mandible on the other.
It is divided into two compartments by the mylohyoid muscle:
1. Sublingual compartment (above the mylohyoid).
2. Submaxillary and submental compartment (below the mylohyoid).
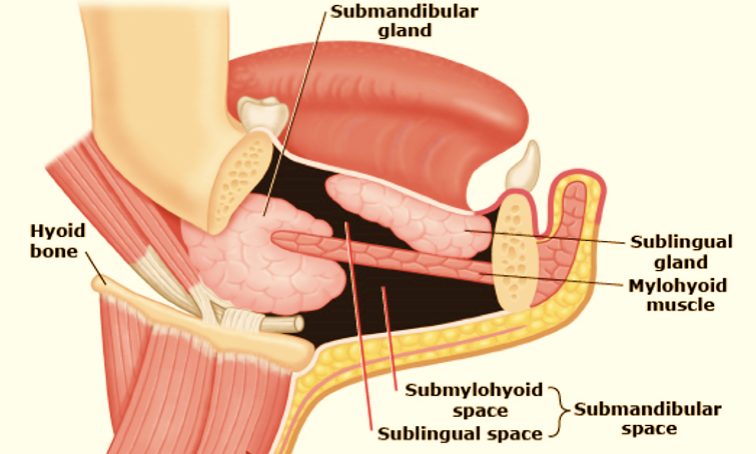
Submandibular space
Most commonly.
1. As a result of alveolar abscess or other dental infections.
2. Suppurative lymphadenitis of the submandibular lymph nodes.
3. Infections from the oral cavity.
1. Ludwig’s angina is caused by mixed infections involving both aerobes and anaerobes.
2. Alpha-haemolytic Streptococci, Staphylococci and Bacteroides groups are common. Rarely Haemophilus influenzae, Escherichia coli and Pseudomonas are seen.

1) Pain, odynophagia and excessive salivation.
2) When the infection is in the sublingual space, the floor of the mouth is swollen.
3) Tongue is displaced downwards.
4) Varying degrees of trismus may be present.
5) Brawny oedematous swelling of the submandibular region.
6) Speech is impaired.
7) Stridor may be present due to laryngeal oedema.
8) As the infection is rapidly spreading, inflammatory oedema may cause suffocation and death.
a) Intravenous antibiotics should be started immediately.
b) Anti-inflammatory drugs are given.
c) Tension of inflammatory exudate must be relieved, and pus must be drained as early as possible. This is done by making a curved incision starting from greater cornu of the hyoid bone to the midline.
d) The mylohyoid may have to be divided if pus is deep to mylohyoid muscle.
e) Once the trismus improves and acute inflammation subsides, dental treatment is necessary to treat the root infection.


a) Spread of infection to the mediastinum causing mediastinitis.
b) Severe stridor due to laryngeal oedema.
c) Septicemia.