
Definition: Tracheostomy is making an opening on the anterior wall of the trachea for establishing an airway.
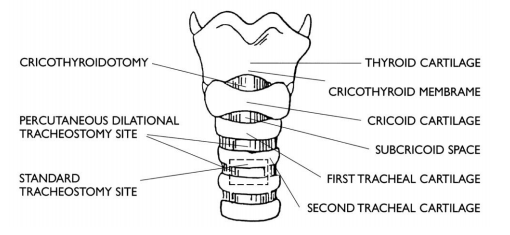
I.High tracheostomy:
This is done about 2 cms above the isthmus of the thyroid gland at the level of 1st tracheal ring. It violates the first ring of trachea so tracheostomy at this site can cause perichondritis of the cricoid cartilage, resulting in subglottic stenosis. Only indication for high tracheostomy is carcinoma of larynx where total larynx is removed and a fresh tracheostome made in a clean area lower down.
II. Mid tracheostomy:
This done at the level of the isthmus of the thyroid gland at the level of 2nd or 3rd tracheal ring. However, the thyroid isthmus needs to be clamped, cut and ligated or retracted upward or downward.
III.Low tracheostomy:
This is done just below the isthmus of the thyroid gland. The 4th tracheal ring in incised. However, one has to be careful not to damage the pleura.
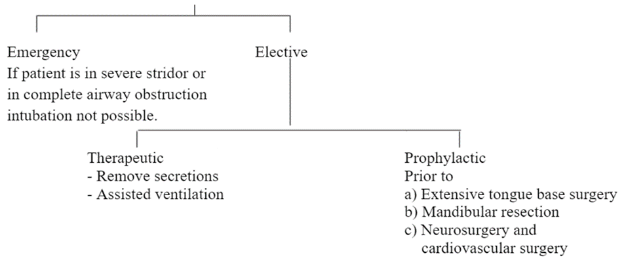
I.Temporary tracheostomy::
Tracheostomy done only for a short period of time. The patient is expected to be weaned off the tracheostomy tube shortly.
II.Permanent tracheostomy::
The patient may need the tracheostomy for a prolonged period of time. Commonly seen in bilateral abductor cord palsy and after laryngectomy surgery.
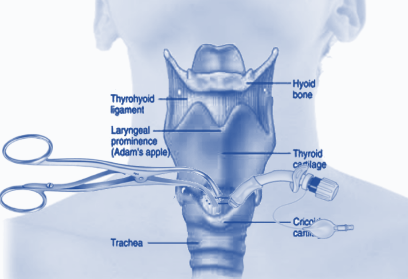
1.It is also called as cricothyrotomy, thyrocricotomy, cricothyroidotomy, inferior laryngotomy, intercricothyrotomy, coniotomy or emergency airway puncture.
2. This is a procedure for opening the airway through the cricothyroid membrane done in emergency situations. .
3.Cricothyroid needle puncture is a procedure where a large-bore intravenous catheter is introduced through the cricothyroid membrane. It is only an emergency procedure till patient is intubated or tracheostomized..
1.This type of tracheostomy is done in ICU where patient is already intubated.
2. It is done under sedation
3. Neck is extended with a pad under the shoulders. Neck is prepared and draped and 1.5–2 cm incision is made 2 cm below the lower border of cricoid. Trachea is exposed by dissection and palpation. Thyroid isthmus is pushed down.
4. Now a small caliber flexible bronchoscope, to which a camera has been attached, is passed through the endotracheal tube to monitor the passage of the needle, guide wire and dilators
5.Entry into the trachea is made between second and third tracheal rings. .
6. After dilatation, tracheostomy tube is inserted.