MÉNIÈRE’S DISEASE
In 1861 Prosper Meniere described a condition characterized by sudden spontaneous episodes of vertigo, nausea, vomiting and fluctuating hearing loss. This is called Meniere’s Disease or endolymphatic hydrops.
Aetiology:
- Age: Peak Incidence is between 35 to 60 year of age.
- Sex: Common in males than females.
- Usually unilateral. Only 10% of the patients have bilateral involvement.
- Vascular insufficiency.
- Idiopathic.
Pathology:
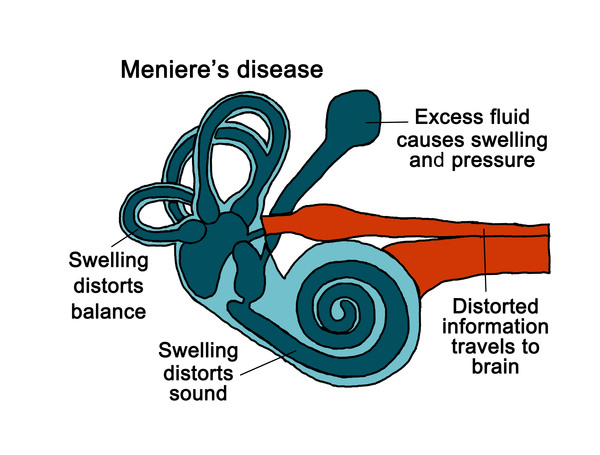
- 1.Overproduction or malabsorption of endolymph, results in endolymphatic hypertension. The endolymphatic hypertension further results in gross enlargement of membranous labyrinth called endolymphatic hydrops.
- 2.Vascular insufficiency may play a role in endolymphatic dysfunction.
Clinical features:
- Early reversible hearing loss
- Established fluctuating hearing loss
- Late non-fluctuating hearing loss
- Vagal stimulation may occur. Patient complains of sweating and pallor. This is seen in acute attacks.
- Recurrent attacks of spontaneous vertigo. Intensity of vertigo increases over a period of minutes and then usually lasts for several hours (20 minutes to 24 hours)
- Tinnitus: It is variable, low pitched, roaring in nature and prominent before an attack. Tinnitus is unilateral and subjective.
- Sensation of heaviness and fullness in the ear.
- Severe anxiety.
- Nystagmus is always present during an attack.
Diagnosis:
- 1. Possible Meniere’s disease-
- Episodic vertigo without hearing loss.
- Sensorineural hearing loss, fluctuating or fixed, with disequilibrium but without definitive episodes.
- Other causes excluded.
- 2. Probable Meniere’s disease-
- One definitive episode of vertigo.
- Hearing loss documented by pure-tone audiogram on at least one occasion.
- Tinnitus or aural fullness on the affected side.
- Other possible causes excluded.
- 3. Definite Meniere’s disease-
- Two or more spontaneous attacks of vertigo (each lasting 20 minutes or longer).
- Hearing loss documented by pure-tone audiogram on at least one occasion.
- Tinnitus or aural fullness on the affected side.
- Other possible causes excluded.
- 4. Certain Meniere’s disease-
- Two or more spontaneous attacks of vertigo (each lasting 20 minutes or longer).
- Hearing loss documented by pure-tone audiogram on at least one occasion.
- Tinnitus or aural fullness on the affected side.
- Other possible causes excluded.
- Histopathological confirmation of the disease.
Investigation:
- Pure tone audiometry: Suggestive of sensorineural hearing loss in the affected ear. It is fluctuating in the early stages.
- Vestibular function test: Electronystagmography shows presence of spontaneous or abnormal nystagmus.
- Glycerol test: Strongly diagnostic of Meniere’s disease.
- General Examination of the patient with neurological examination.
- BERA is used to differentiate unilateral acoustic tumors. Normal in Meniere’s disease.
- Electrocochleography: Here ratio of summating potential (SP) to action potential (AP) ratio is greater than 30%.
Treatment:
1.General:
a) Stop alcohol, Smoking.
b) Monitor blood pressure.
c) Sound Sleep.
2. Medical:
a) Reduce sodium intake.
b) Diuretics Furosemide 10-70 mg/day.
c) Vestibular ablation by injection Streptomycin.
d) Vasodilators, Betahistine.
e) Calcium channel blockers: Useful in some patients not responding to the above treatment.
f) Sedatives to relieve anxiety.
g) Labyrinthine sedatives with antiemetics used in acute period.
h) Anti-histaminic- Act as vestibular suppressants.
3. Surgical:
a) Chemical Labyrinthectomy of inner ear by injection gentamycin.
b) Ultrasonic ablation of the inner ear.
c) Endolymphatic Sac decompression. Helps to prevent the accumulation of the endolymph.
d) Vestibular neurectomy.
e) Labyrinthectomy: It comprises of destruction of the labyrinth to relieve the symptoms.