
They are benign, very vascular and biologically aggressive tumors, originating almost exclusively from posterior nasal and nasopharyngeal region in adolescent males.
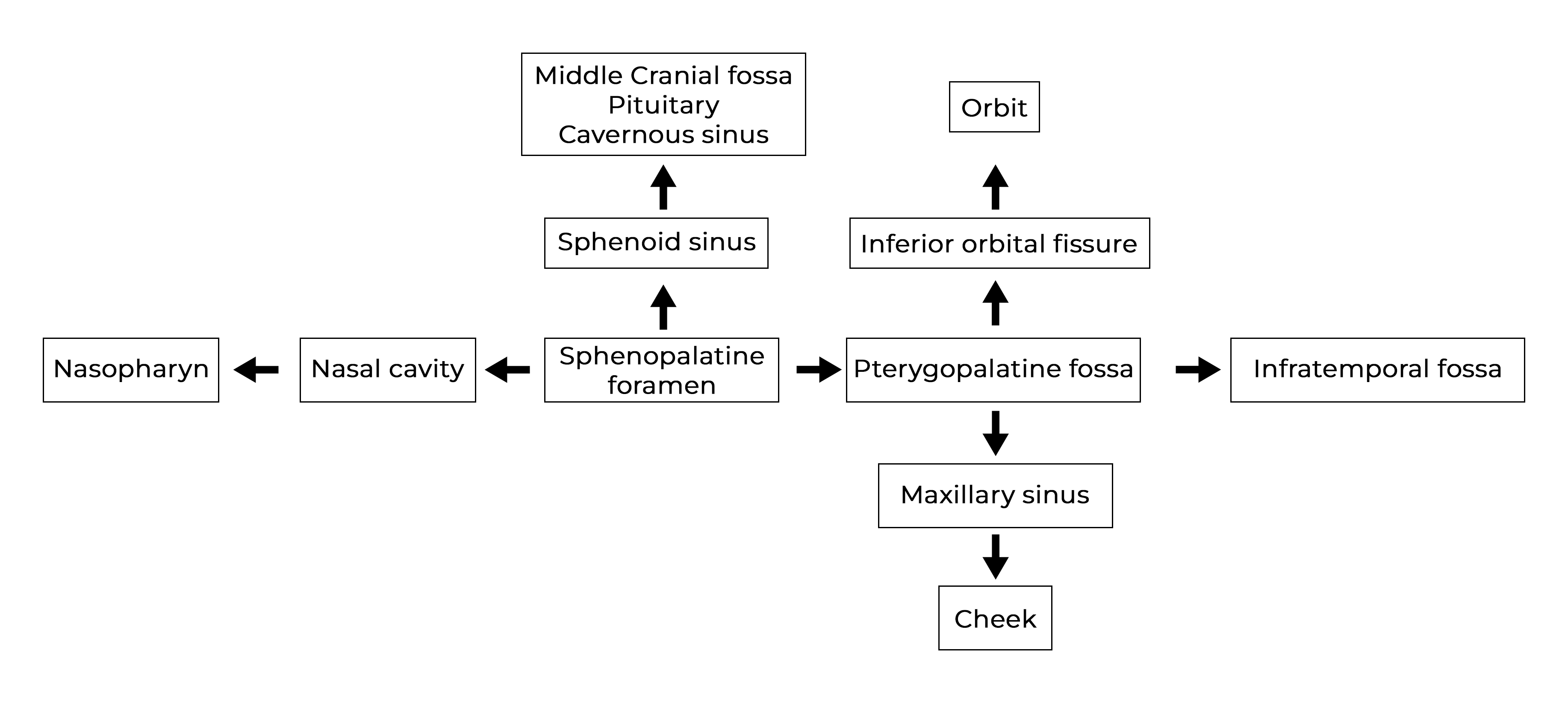

The tumour usually arises from the sphenopalatine foramen or the posterior wall of the nasal cavity with adjoining superolateral wall. The blood vessels are devoid of tunica media, hence the bleeding is torrential.
Major arterial supply is from the ipsilateral internal maxillary artery. Collateral supply is from the ascending pharyngeal artery and branches of internal carotid artery.
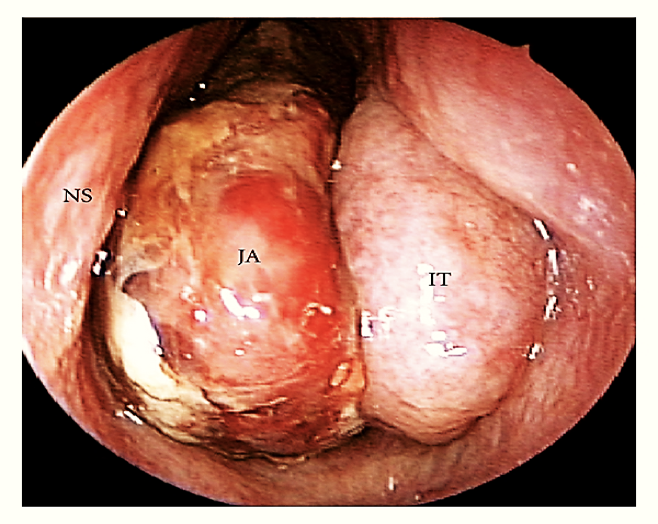
Nasopharyngeal angiofibroma in left nasal cavity.

CT scan PNS showing mass in nasal cavity, nasopharynx, pterygopalatine fossa with distortion of nasal septum, medial and posterior wall of maxillary antrum.
1) Surgical excision by: